

Hold the guilt! A new study shows — once again — that the purported benefits of breastfeeding are actually benefits of privilege. Breastmilk has little if anything to do with it.
That was already demonstrated powerfully in the 2014 Colen study, Is Breast Truly Best? Estimating the Effects of Breastfeeding on Long-term Child Health and Wellbeing in the United States Using Sibling Comparisons. The answer was “No.”
The authors looked at breastfeeding vs. bottlefeeding WITHIN families by comparing siblings who were fed differently. In that way they eliminated the impact of race and socio-economic status. When they did, there was no difference between breastfed and bottlefed children.
It isn’t breastfeeding that improves infant health; it is privilege.
Now an even more ingenious study has confirmed those finding, The best of intentions: Prenatal breastfeeding intentions and infant health. The authors correct for the impact of race and socio-economic status by focusing on intention to breastfeeding instead of breastfeeding itself.
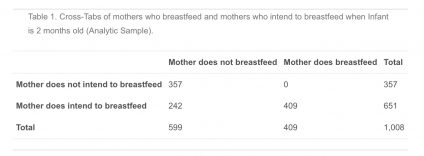
The authors looked at more than 1000 women and categorized them based on whether they intended to breastfeed or not.
They noted:
…Approximately one-third of mothers who intend to exclusively breastfeed are able to achieve this goal. There are several exogenous factors that may prevent mothers from fulfilling their intentions. For example, biological barriers include low milk supply, pain, infections (mastitis), or clogged milk ducts. The baby may have a poor latch, be an ineffective nurser, or have food intolerances… Some factors may act as both an influence on a mother’s intentions as well as her ability to realize those intentions. For example, maternal employment, lack of social support, limited knowledge, or limited access to professional support such as lactation consultants may first undermine intentions and then breastfeeding success.
In sum, prenatal breastfeeding intentions may be an important factor in examining the relationship between breastfeeding and infant health as they help us to overcome a key identification challenge in measuring the effect of breastfeeding on infant health: that the same characteristics that lead a mother to breastfeed may also lead to an infant having improved health. (my emphasis)
They looked at three infant health outcomes: ear infections, respiratory syncytial viruses (RSV), and antibiotic usage in the infant’s first year.
They found that women who intended to breastfeed had infants with better health outcomes even if they DIDN’T breastfeed!
An infant born to a mother who intended and did breastfeed had approximately 35% (or 0.165) fewer ear infections than infants born to mothers who had no intention of breastfeeding, but an infant born to a mother who intended and did not breastfeed had approximately 29% (or 0.136) fewer ear infections compared to the same omitted group. There is no statistically significant difference in ear infections between intending mothers who did and did not breastfeed.
Next, we examine the RSV outcome. Compared to infants whose mothers did not breastfeed and did not intend to do so, infants with mothers who intend and do breastfeed are 83% less likely to have an episode of RSV in their first year of life (a marginal effect of 0.056 fewer episodes). The coefficient for infants born to mothers who intended but did not breastfeed is not significant but suggests a qualitatively large difference (36% less likely to have an RSV diagnosis, which is 0.024 fewer diagnoses). This substantial percent difference (83% vs 36%) is likely due to RSV being a rare outcome; only 7% of mothers in our sample reported RSV.
Finally, we focus on antibiotic usage, and our analysis suggests that prenatal intentions are negatively linked to incidents of antibiotic use. The infants whose mothers intended and did breastfeed had 38% fewer incidents where antibiotics were used, compared to infants of non-intending mothers, while infants whose mothers intended but did not breastfeed had 40% (or 0.293) fewer incidents where antibiotics were used compared to infants of non-intending mothers. Both coefficients are statistically different from the omitted group, but the difference between breastfeeding and formula-feeding mothers who intended to breastfeed is insignificant.
What’s going on?
The authors investigated differences in nutrition knowledge and sources between groups of mothers and found that women who intended to breastfeed but did not were very similar to women who intended to breastfeed and were able to do so. Both differed in important ways from women who had not intended to breastfeed. It is the differences between mothers that are responsible for the differences in outcome, not breastfeeding.
The authors summarize:
[O]ur findings help to contextualize the finding that “breast is best,” and add nuance to a body of literature on the benefits of breastfeeding for infant health. Although we do not dispute that breastmilk is an excellent source of nutrition, our results suggest that formula offers similar health benefits for our relatively advantaged sample of infants, once we take prenatal intentions into account. (my emphasis)
The authors amplify their findings in an interview in the mainstream press:
“By sinking so much energy into getting moms to breastfeed, we miss something very important: That access to health care and the ability to take medical advice is critically important to a mother and her infant,” said Raissian. “By exploring factors influencing better infant health outcomes, information from the study helps contextualize the trade-offs that a lot of mothers have to make when deciding how to feed their children.”
It isn’t breastfeeding that improves infant health; it is privilege.
That explains why efforts to promote breastfeeding have been spectacular failures when it comes to improving outcomes. With the exception of premature babies, breast milk doesn’t have many benefits at all.
There is no correlation between breastfeeding rates and infant mortality rates. Countries with the highest infant mortality rates have the highest breastfeeding rates and countries with the lowest breastfeeding rates have the lowest infant mortality rates. Increasing breastfeeding rates within a country has no impact on infant mortality or other health outcomes. The promised monetary savings have also failed to materialize.
The authors have elegantly demonstrated that breastfeeding is a proxy for privilege. It is intention to breastfeed that leads to improved outcomes, not breastfeeding itself.
