
One of the great ironies of natural childbirth is that the same folks who get hysterical about the possibility that a baby’s umbilical cord is cut early, potentially depriving him or her of oxygen, blithely ignore of what happens to a baby who isn’t getting enough oxygen during labor.
What will happen to your baby if he or she is chronically deprived of oxygen during the hours of labor — because the placenta isn’t transmitting it fast enough (placental insufficiency, postdates pregnancies) or your baby is deprived of oxygen acutely (a tight nuchal cord, severe shoulder dystocia, breech with a trapped head, placental abruption, ruptured uterus during attempted VBAC).
The new paper Pathophysiology of foetal oxygenation and cell damage during labour is highly technical, but in its own way quite chilling.
The authors set the stage:
[pullquote align=”right” color=”#b27d27″]Your baby must have a steady supply of oxygen for cells to work properly.[/pullquote]
All human cells require oxygen and glucose to maintain aerobic metabolism and for energy production. The foetal oxygen requirement is determined by foetal size, activity and essential metabolic processes. During foetal life, the oxygen supply is dependent entirely on maternal respiration and circulation, placental perfusion, gas exchange across the placenta and the umbilical and foetal circulations. If the supply and requirement are in balance, the foetus has adequate oxygen to metabolise glucose aerobically to produce the energy required for organ function…
During the human birth process, the foetus is squeezed through the birth canal over a period of up to several hours, during which the head sustains considerable pressure and the foetus is intermittently deprived of oxygen. A reduced oxygen supply is often categorised into three types: (1) hypoxaemia, involving a reduced oxygen in the arterial blood, but where cell and organ function are not usually affected; (2) hypoxia, with reduced oxygen and subsequent anaerobic metabolism, mainly in the peripheral tissues; and (3) asphyxia, where the hypoxia extends to the central organs e the heart, brain and adrenal glands e and potentially leads to metabolic acidosis.
… Asphyxia is one of the main causes of neonatal and childhood mortality and morbidity, and it has been associated with neonatal death, hypoxic-ischaemic encephalopathy (HIE), seizures, intraventricular haemorrhage, cerebral palsy (CP) and delayed development.
In other words, your baby must have a steady supply of oxygen for cells to work properly. A baby can tolerate the reduced oxygen supply during contractions, but only if the placenta is transferring enough between contractions. What happens when that steady supply is compromised by a poorly functioning placenta?
First:
…[F]oetal metabolism switches to anaerobic. This leads to a decrease in pH, accumulation of lactate and an increase in the base deficit (BD)…
According to the international consensus, metabolic acidosis in the umbilical cord arterial blood at birth is defined as umbilical cord pH
When there isn’t enough oxygen available, fetal cells switch to an alternate method of metabolism that produces lactate, which accumulates and makes the blood acidic. This is similar to the process that might happen to you during vigorous exercise. In adults it causes cramps, nausea and weakness. It’s unlikely to be pleasant for your baby.
If the process continues, your baby will begin to asphyxiate (suffocate).
The authors note:
Foetal asphyxia almost always occurs as a result of a gradual insufficiency in the umbilical blood flow or insufficient uterine blood flow, and in most cases, it is attributable to a reduction in gas exchange for variable time periods. However, a sudden complete cessation of oxygen delivery to the foetus as a cause of asphyxia is clinically rare, but often catastrophic.
Your baby will attempt to protect him/herself.
This includes changes in FHR, reduction of oxygen consumption secondary to the cessation of non-essential functions such as body and eye movements, reduction of body temperature
and centralisation (redistribution of cardiac output to preferentially perfuse vital organs such as the heart, brain and adrenal glands (Fig. 3); and a switch to anaerobic cellular metabolism first in the peripheral organs and subsequently in the central organs). The degree to which these mechanisms are effective in preventing asphyxia depends upon the overall health of the foetus and the placenta, as well as the duration, frequency and intensity of the hypoxaemic event(s).
To conserve oxygen, your baby will stop moving in, lower his or her body temperature, and shunt blood away from most organs to send oxygenated blood preferentially to the heart and brain in a desperate attempt to stay alive.
But:
As asphyxia progresses, the foetus loses the ability to protect its vital organs, and there are subsequent further decreases in the blood flow to the heart and the brain. Decomposition with severe metabolic acidosis is associated with a reduction of the arterial pressure due to a decrease in the cardiac output, and ultimately a decrease in the cerebral blood
flow. Thus, the combination of asphyxia and ischaemia due to hypotension and hypoperfusion results in decreased cerebral oxygen consumption and, if sustained, hypoxic brain damage, organ system failure and, ultimately, foetal death.
The brain and the heart and ultimately your baby him/herself begins to die.
The damage does not end if your baby is born alive. Many natural childbirth and homebirth “success” stories imply that if a baby is successfully resuscitated at birth, the problem has been solved. Nothing could be further from the truth.
When the tissue is reoxygenated and reperfused, energy-rich phosphates are rapidly replenished. However, reoxygenation entails the initiation of complex chains of events that result in secondary energy failure and neurotoxicity. The neurotoxicity in the second phase starts by the generation of oxygen derived free radicals and an excess of excitatory amino acids This takes place at 2-6 h after the primary insult, as the restoration of the cerebral blood flowincreases the pO2 in the tissues …
Another significant component affecting the progression of foetal brain injury is the cerebral inflammatory response following hypoxiceischaemic insults. This inflammation is generated by both the activation of local inflammatory cells in the affected brain tissue and the recruitment of circulating immune cells.
The damage to your baby’s brain continues to get worse even though he or she is now getting enough oxygen and looks fine. There is evidence that the bulk of the permanent damage to your baby’s brain will happen in the hours after birth, not during the actual oxygen deprivation. That’s why high tech resuscitation often involves brain cooling. The idea is to decrease the metabolic rate during those critical hours when your baby’s injured brain is producing toxic substances that harm brain cells, and thereby minimize the inevitable additional damage.
The damage may have a long term impact on your baby:
… [H]ypoxic damage typically afflicts the grey matter … The resulting clinical syndrome may take several forms, but two major syndromes can be schematically described. First, when the lack of oxygen develops gradually, the resulting clinical picture in surviving neonates after severe hypoxia-ischaemia is an acute and transient failure of kidney and liver functions together with chronic brain injuries… The neonate shows the typical signs of severe brain injury, and the head does not grow during the following months (microcephaly), and a typical CP syndrome develops with severe spastic paralysis of all four extremities. In the second major syndrome after acute severe hypoxia, the typical brain injury is severe damage to the basal ganglia with sparing of the cerebral cortex… The clinical picture in typical cases is of a child with a normal head circumference and often well-preserved developmental functions, but with gross impairment of motor coordination and balance, and consequently of their total motor performance…
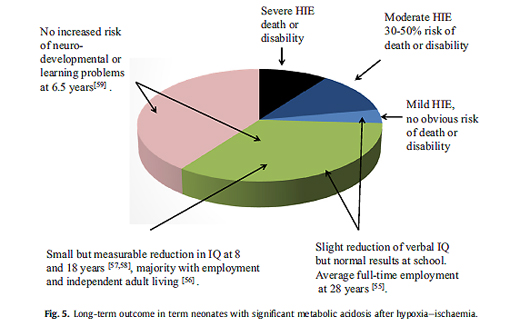
So if your baby experienced ongoing oxygen deprivation during labor the result may be severe brain injury affecting all aspects of function. Your baby will be severely handicapped both physically and intellectually. If your baby was temporarily deprived of oxygen because of an acute event like severe shoulder dystocia, he or she may have normal intellectual function but impaired motor function, typically known as cerebral palsy.
The authors provide a pie chart of outcomes:
How can you protect your baby? The best way is fetal monitoring during labor, either electronic fetal monitoring or intermittent listening (auscultation) following a rigorous protocol. Fetal monitoring, particularly electronic monitoring, has a high false positive rate. That means that it may indicate distress when your baby is not actually oxygen deprived. It does, however, have a low false negative rate, meaning that if your baby’s heart rate monitoring is normal, your baby is very likely to be safe.
A high false positive rate means that a lot of babies are rescued (by emergency C-section, forceps or vacuum) who were never in any trouble. On the other hands, it means that if there is even the slightest indication that your baby’s brain is at risk, everything will be done to prevent injury.
Of course, you could always opt not to monitor at all and “trust” that your baby will survive birth unscathed. Ironically, natural childbirth advocates, the folks who are most concerned with maximizing a child’s intellectual potential and health by breastfeeding, making their own organic baby food, and avoiding any toxins, are most likely to put their babies at risk of the biggest toxin of them all: oxygen deprivation during labor.
