

Below are the characteristics of two types of pain relief in labor. Guess which one is favored by midwives.
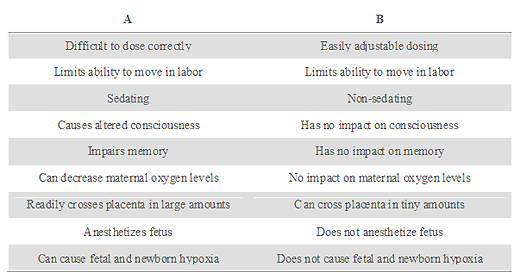
If you guessed “B,” you’d be wrong.
True, it is easily adjustable, non sedating, has no impact on memory or oxygen levels and crosses the placenta in miniscule amounts if at all. But it’s the dreaded epidural and it’s bad, bad, bad.
“A” is, in fact, favored by midwives and used extensively by midwives around the world at home and in the hospital. Indeed, many midwives believe it is perfectly compatible with natural childbirth despite the fact that it is most certainly a drug, marketed by a pharmaceutical company, is difficult to dose effectively, causes sedation and impaired memory, and readily crosses the placenta in large amounts where it sedates the baby.
Shocked? You shouldn’t be. Drug “A” is nitrous oxide and American midwives are clamoring for its use.
A new patient handout prepared by the Journal of Midwifery and Women’s Health expounds on the virtues of nitrous.
… Many women in Europe and other countries, such as Canada and Australia, use it to help cope with pain in labor. It is so common that in some countries as many as 8 in 10 women use nitrous oxide to help with labor pain. Women in these countries have been using this method of pain relief in labor safely for many years. Nitrous oxide hasn’t been used as often in the United States, but that is changing.
The handout acknowledges that nitrous produces altered consciousness and distorted memory, but apparently does not consider that a problem. The handout glosses over the impact of nitrous on the baby:
Nitrous oxide is the only pain relief method used for labor that is cleared from your body through your lungs. As soon as you pull the mask away, the effect of breathing the gas is gone within a few breaths. No extra monitoring is needed for you or the baby because you are using nitrous oxide. If you did get too sleepy, a monitor to check your oxygen levels might be placed on your finger. Nitrous oxide is safe for your baby, so if your baby’s heart rate is being checked intermittently (off and on) rather than continuously (all the time) with a fetal monitor, that is still okay…
Midwives are apparently unconcerned that nitrous crosses the placenta easily and in large amounts, producing sedation and altered consciousness in the baby. In fact, it would be quite accurate to state that nitrous “drugs” the baby whereas epidurals do not.
What’s the impact of nitrous on breastfeeding and newborn behavior? That’s not clear because very little research has been undertaken on the impact of nitrous on the newborn.
So by every parameter we can measure, nitrous has far more impact on women and babies than an epidural, yet nitrous is “good” and epidurals are “bad.” What accounts for this paradox?
It’s simple: midwives can administer nitrous, but lack the skills and training to administer epidurals.
All the pious wailing about the effects of epidurals are nothing more than hypocrisy. It really makes no difference to midwives whether women use “drugs” in labor to relieve pain, even if those drugs limit ability to move in labor, alter consciousness, impair memory, decrease oxygen levels, readily cross the placenta and sedate the fetus … just so long as they can administer the drugs.
