

The annual meeting of the Society for Maternal-Fetal Medicine is currently being held in Dallas. Two different papers will be presented today, both of which highlight the increased risks of homebirth.
The first is Neonatal outcomes associated with intended place of birth: birth centers and home birth compared to hospitals (abstract 65) by Cheng, Snowden and Caughey. According to the authors:
This was a retrospective cohort study of singleton live births that occurred in 2008 in the U.S. that had specified birthing facility information. Deliveries were categorized by location of occurrence: hospitals, birthing centers, or intended home births…
What did they find?
While the risk of cesarean delivery was much lower for women who delivered/or intend to deliver outside of hospitals (0.02-4% vs. 24%, <0.001), the odds of 5-minute Apgar score <7 and neonatal seizure was significantly higher for intended home births compared to hospital birth.
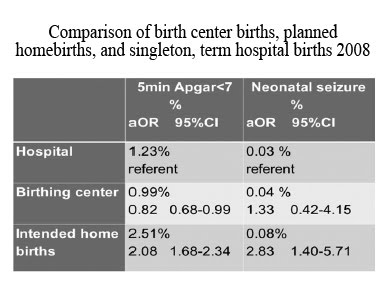
In other words, while homebirth has a dramatically lower C-section rate, the price is double to triple the rate of birth asphyxia. This study actually substantially underestimates the risk of these serious complications at homebirth because it compares homebirth to all risk hospital birth instead of low risk hospital birth.
The second study is entitled Does planned home birth affect neonatal mortality? (abstract 563) by Joel Larma.
This is a population based retrospective cohort study of all births between 37 and 42 weeks gestation using the National Health Center for Vital Statistics 2005 Linked Birth/Infant Death Cohort Data Set. The primary outcome was neonatal mortality and the primary predictor was planned home birth. The referent group for the regression model was births that occurred in a hospital…
The authors did not separate homebirths attended by CNMs from homebirths attended by non-nurse midwives. The analysis showed that homebirth more than doubled the risk of neonatal death. This actually underestimates the risk because it compares homebirth to term hospital birth in women without pre-existing medical conditions, but apparently includes hospital births with pregnancy complications.
The adjusted OR for neonatal mortality among individuals having a planned home birth was 2.32 (95% CI 1.33, 4.06) after controlling for the aforementioned covariates [age, race, marital status, education, prenatal care, tobacco use, composite medical comorbidities].
CONCLUSION: The odds of neonatal mortality are significantly increased among those individuals having a planned home birth compared to those individuals giving birth in the hospital.
The amount of data on planned homebirth is slowly growing and the findings are remarkably robust. These studies, like all the existing scientific evidence, state and national statistics show that homebirth doubles or triples the rate of neonatal death and other adverse outcomes, and that the analyses almost certainly underestimate the real increased risks at homebirth.
addendum: These studies underestimate the risk even further because, as far as I can determine, bad outcomes that occurred after homebirth transfer are included in the hospital group and removed from the homebirth group. The real number of bad outcomes and deaths is higher than what the authors were able to determine.
