

Natural childbirth advocates often appear to be nothing more than a bunch of parrots. One of them makes up something and the rest of them mindlessly repeat it.
Consider the issue of maternal mortality. Fittingly, Ina May Gaskin, the biggest fraud in the world of NCB advocacy, misconstrued the most basic information (possibly deliberately) and fashioned the biggest lie. And once she made it up, Ina May played it for all it was worth.
In creating and promoting this lie, Gaskin harkens to a classic technique in pseudoscience. As described by Paul Wolpe in The Holistic Heresy: Strategies of Ideological Challenge in the Medical Profession an attack by purveyors of “alternative” medicine on an established discipline in medicine includes specific elements. The first is that the critic:
must portray the discourse as in crisis, must provide an alternative ideology to rescue the discourse, must legitimize their ideology through appeal to a reframed historical myth, and must portray the orthodoxy as a betrayer of the discourse.
According to Gaskin, rising US maternal mortality is an indication that contemporary obstetrics is in crisis. There’s just one problem: US maternal mortality is not rising.
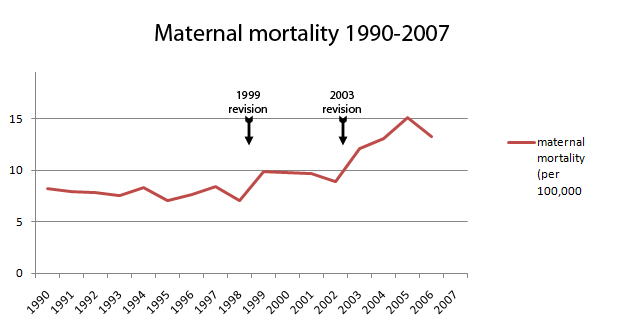
In 1999 and again in 2003, the standard birth certificate was redesigned to capture all maternal deaths by expanding the maternal mortality criteria. Not surprisingly, maternal mortality appeared to rise as a result. There is no evidence that it actually rose (indeed the CDC has established that it did not rise) but that didn’t matter to Gaskin. She grabbed the issue and exploited it to promote homebirth midwifery. In a public relations master stroke, she even created a quilt (consciously modeled on the AIDS Quilt) to foster the illusion that the maternal mortality rate was rising and that modern obstetrics was the cause.
In May, Amy Romano, CNM of the Childbirth Connection parroted this falsehood in honor of Mother’s Day. Now Kimmelin Hull of Lamaze has jumped on the bandwagon. Hull, who (as she never tires of telling us) is working on an master’s in public health, ought to know better. However, the opportunity to criticize contemporary obstetrics is just too tempting, facts be damned.
Hull begins by parroting the lie that US maternal mortality has been rising. Hull quotes the WHO, the CDC, Amnesty International, and (of course) Gaskin, but she neglects to quote the specific studies that show that the apparent increase in maternal mortality is due to the birth certificate revisions.
From Deaths: Final Data for 2008:
Research done on this issue indicates that this increase represents an improvement in identifying maternal deaths. For example, a study in Maryland that used multiple data sources as the standard showed an improvement (from 62 percent to 98 percent) in identifying maternal deaths after adoption of a pregnancy checkbox item consistent with the 2003 standard certificate.
And Changes in Pregnancy Mortality Ascertainment: United States, 1999–2005:
The maternal mortality ratio increased significantly from 11.6 in 1995–1997 to 13.1 for 1999–2002 and 15.3 in 2003–2005 … Vital statistics identified significantly more indirect maternal deaths in 2002–2005 than in 1999–2002. Between 2002 and 2005, mortality ratios increased significantly among 19 states using the revised death certificate with a pregnancy checkbox; ratios did not increase in states without a checkbox. (my emphasis)
Having parroted the lie, Hull then proceeds to parrot the claim that contemporary obstetrics is in crisis:
… Perhaps then, the simplistic question to ask is, “If we are spending so much money each year on maternity care, why is the maternal death rate in our country climbing when expenditures—estimated to be in the hundreds of billions of dollars—on other health conditions, such as cardiovascular disease, are resulting in declining death rates?”
Then, nonsensically, Hull parrots the assertion that midwifery theory is the answer:
… By encouraging the perspective that pregnancy and birth are inherently normal, healthy processes (as opposed to disease/disease states) the eventual clinician is more likely to approach patients with a sense of trust in the germane mechanics associated with pregnancy and birth as opposed to a pessimistic assumption that each pregnant patient is a “ticking time bomb” to be weary of.
What? The solution to an increase in maternal mortality is to trust birth? That makes no sense. But making sense, like the truth itself, is irrelevant to the NCB parrots.
